What happened?
Vessel A departed from Singapore Eastern Petroleum “A” anchorage (AEPA) intending to join the eastbound lane of the TSS at the precautionary area. Meanwhile, Vessel B was proceeding in the westbound lane of the TSS, following the general traffic flow towards Pilot Eastern Boarding Ground “C” (PEBGC). Despite VTIS (Vessel Traffic Information Service) advising Vessel A to cross the westbound lane only after Vessel B had passed, Vessel A made a significant starboard alteration of course whilst approaching Vessel B, resulting in a collision.
Why did it happen?
Vessel B reduced speed to adjust its Estimated Time of Arrival (ETA) at PEBGC, during which Vessel C overtook it on the port side. At this time, Vessel A’s intention was to follow Vessel B’s stern, adjusting its heading for crossing the TSS. However, as Vessel A drew closer to Vessel B, it made a significant starboard alteration.
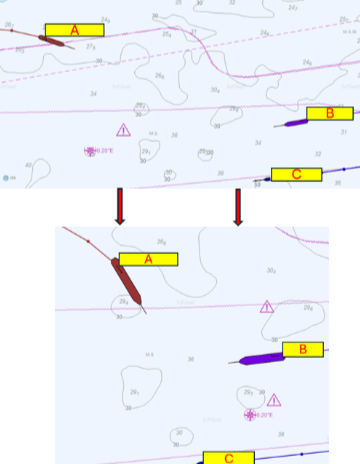
Analysis suggests that Vessel A's bridge team mistakenly tracked Vessel C’s path to cross the TSS instead of Vessel B. When Vessel C completed its overtaking of Vessel B and became visible to Vessel A, the bridge team lost situational awareness of Vessel B’s position and shifted attention from monitoring Vessel B to following Vessel C’s stern for the TSS crossing (see Figure 1).
Bridge Watch Level
The bridge team on Vessel A consisted of the Master, Officer of Watch (OOW/Second Officer), and Helmsman, which was at manning level 3. During the pilot disembarkation, the Second Officer escorted the pilot to the ladder, temporarily reducing the bridge team to level 2, with no dedicated lookout maintained.
Look Out
The collision’s primary cause was attributed to the absence of a proper lookout on both vessels. The Masters and OOWs failed to maintain adequate situation awareness of the developing close-quarter situation. The master of Vessel A, without conducting a comprehensive assessment, attempted to cross the TSS while following an incorrectly identified vessel. Simultaneously, Vessel B’s bridge team failed to properly evaluate the crossing situation and did not detect Vessel A’s change in aspect at close range. Critically, there was no monitoring or assessment of Vessel A’s movement
Conclusion and recommendations
The collision between Vessel A and Vessel B resulted from a combination of poor bridge team management and inadequate situational awareness. The temporary reduction in bridge manning during pilot disembarkation, coupled with the failure to maintain proper lookout, led to critical errors in vessel identification and traffic assessment for Vessel A. Vessel A's bridge team's misidentification of the vessel to follow, and Vessel B's failure to monitor the developing situation, ultimately resulted in the collision.
To prevent recurrence, it is recommended that: